
Sam Parnia MD has a highly sought after medical speciality: resurrection. His patients can be dead for several hours before they are restored to their former selves, with decades of life ahead of them.
Parnia is head of intensive care at the Stony Brook University Hospital in New York. If you'd had a cardiac arrest at Parnia's hospital last year and undergone resuscitation, you would have had a 33% chance of being brought back from death. In an average American hospital, that figure would have fallen to 16% and (though the data is patchy) roughly the same, or less, if your heart were to have stopped beating in a British hospital.
By a conservative extrapolation, Parnia believes the relatively cheap and straightforward methods he uses to restore vital processes could save up to 40,000 American lives a year and maybe 10,000 British ones. Not surprisingly Parnia, who was trained in the UK and moved to the US in 2005, is frustrated that the medical establishment seems slow and reluctant to listen to these figures. He has written a book in the hope of spreading the word.
The Lazarus Effect is nothing short of an attempt to recast our understanding of death, based on Parnia's intimate knowledge of the newly porous nature of the previously "undiscovered country from which no traveller returns". His work in resuscitation has led him logically to wider questions of what constitutes being and not being. In particular, he asks what exactly happens, if you are lying dead before resuscitation, to your individual self and all its attendant character and memories – your "soul", as he is not shy to call it – before it is eventually restored to you a few hours later?
When I meet Parnia, he is not long off the plane from New York after a night flight with his wife and baby daughter, and the particular revival he is craving is the miracle of strong coffee. He is both forthright and softly spoken, full of careful zeal for his findings. As I sit across the table from him, he can make even the most extraordinary claim seem calmly rational. "It is my belief," he says, "that anyone who dies of a cause that is reversible should not really die any more. That is: every heart attack victim should no longer die. I have to be careful when I state that because people will say, 'My husband has died recently and you are saying that need not have happened'. But the fact is heart attacks themselves are quite easily managed. If you can manage the process of death properly then you go in, take out the clot, put a stent in, the heart will function in most cases. And the same with infections, pneumonia or whatever. People who don't respond to antibiotics in time, we could keep them there for a while longer [after they had died] until they did respond."
Parnia's belief is backed up by his experience at the margin of life and death in intensive care units for the past two decades – he did his training at Guy's and St Thomas' in London – and particularly in the past five years or so when most of the advances in resuscitation have occurred. Those advances – most notably the drastic cooling of the corpse to slow neuronal deterioration and the monitoring and maintenance of oxygen levels to the brain – have not yet become accepted possibilities in the medical profession. Parnia is on a mission to change that.
The one thing that is certain about all of our lives, he says, is that we will all eventually experience a cardiac arrest. All our hearts will stop beating. What happens in the minutes and hours after that will potentially be the most significant moments of our biography. At present, the likelihood is, however, that in those crucial moments we will find ourselves in the medical environment of the 1960s or 1970s.
The kind of CPR (cardiopulmonary resuscitation) that we are familiar with from medical dramas – the frenzied pumping of the chest – remains rooted, Parnia claims, in its serendipitous discovery in 1960. It remains a haphazard kind of procedure, often performed more in hope than anticipation. Partly, this is a question of personnel. Parnia is quietly maddened by the worldwide hospital habit, in the event of death, to send the most junior of doctors along "to have a go at CPR". It is as if hospital staff have given up before they have started.
"Most doctors will do CPR for 20 minutes and then stop," he says. "The decision to stop is completely arbitrary but it is based on an instinct that after that time brain damage is very likely and you don't want to bring people back into a persistent vegetative state. But if you understand all the things that are going on in the brain in those minutes – as we now can – then you can minimise that possibility. There are numerous studies that show that if you implement all the various resuscitation steps together you not only get a doubling of your survival rates but the people who come back are not brain damaged."
In Parnia's ideal world, the way that people are resuscitated would first take in the knowledge that machines are much better at CPR than doctors. After that, he suggests, the next step is "to understand that you need to elevate the level of care". The first thing is to cool down the body to best preserve the brain cells, which are by then in the process of apoptosis, or suicide.
At the same time, it is necessary to keep up the level of oxygen in the blood. In Japan, this is already standard practice in emergency rooms. Using a technique called an ECMO, the blood of the deceased is siphoned out of the body, put through a membrane oxygenator and pumped round again. This buys the time needed to fix the underlying problem that caused the person to die in the first place. If the level of oxygen to the brain falls below 45% of normal the heart will not restart, Parnia's research shows. Anything above that and there is a good chance.
Potentially, by this means, dead time can be extended to hours and there are still positive outcomes. "The longest I know of is a Japanese girl I mention in the book," Parnia says. "She had been dead for more than three hours. And she was resuscitated for six hours. Afterwards, she returned to life perfectly fine and has, I have been told, recently had a baby."
It was a truncated version of this process, at the London Chest Hospital, that allowed the Bolton footballer Fabrice Muamba to be restored to life after he collapsed on the pitch at White Hart Lane last year. Parnia watched the events unfold on TV and subsequently kept on reading that Muamba had been, for up to an hour, "dead" – but always in quotation marks. He laughs. "Journalists have invented a new term, 'clinically dead'. I don't know what that term means. But the fact is Muamba was dead. And it was not by a miracle he was brought back to life, it was by science."
One of the stranger things you realise in reading Parnia's book is the idea that we might be in thrall to historical perceptions of life and death and that these ultimate constants have lately become vaguer than most of us would allow. The other strand of Parnia's research, in which he leads a team at Southampton University, is into what most people tend to call "near-death experiences" and what he calls "actual death experiences". Parnia has talked to many people about what they recall experiencing while they were dead in his intensive care unit. About half claim to have clear recollections, many of which involve looking down on the surgical team at work on their body or the familiar image of a bright threshold or tunnel of light into which they were being drawn. Parnia has been collecting detailed accounts of these experiences for four years. I ask what conclusions he has drawn.
He suggests he is agnostic about the source of these subjective memories, as he is about questions of mind and matter. "When I first got interested in these mind/body questions, I was astonished to find that no one had even begun to put forward a theory about exactly how neurons in the brain can generate thoughts," he says. "We always assume that all scientists believe the brain produces the mind, but in fact there are plenty who are not certain of that. Even prominent neuroscientists, such as Sir John Eccles, a Nobel prizewinner, believe that we are never going to understand mind through neuronal activity. All I can say is what I have observed from my work. It seems that when consciousness shuts down in death, psyche, or soul – by which I don't mean ghosts, I mean your individual self – persists for a least those hours before you are resuscitated. From which we might justifiably begin to conclude that the brain is acting as an intermediary to manifest your idea of soul or self but it may not be the source or originator of it… I think that the evidence is beginning to suggest that we should keep open our minds to the possibility that memory, while obviously a scientific entity of some kind – I'm not saying it is magic or anything like that – is not neuronal."
Does he have a religious faith?
"No," he says, "and I don't have any religious way into this. But what I do know is that every area of inquiry that used to be tackled by religion or philosophy is now tackled and explained by science. One of the last things to be looked at in this way is the question of what happens when we die. This science of resuscitation allows us to look at that for the first time."
While those more esoteric studies go on, Parnia wants to ensure that more and more people are successfully returned from death to tell whatever tales they can. "I still have colleagues in ICU who say, 'I don't know why we are doing all this stuff'," he says. "Not long ago, I went for a job interview in New York at a teaching hospital and I was told if a patient comes in and has a cardiac arrest and they end up in the cardiac care unit they will be cooled, but if they end up in the intensive care unit the doctor in charge doesn't believe in it. He thinks it blocks his beds so he won't do it. I don't see this as negligence exactly because there is, as yet, no authority telling us this is the standard we should use. But surely there should be." All of this, I say, must have had a powerful bearing on Parnia's own sense of mortality. Is he comforted or made paranoid by his work?
He suggests that the experience of talking to people who have returned from dying serves only to enhance his curiosity about the process they have undergone, and which he has sometimes helped to reverse. Other than that, he says: "In ICU, I see people dying every day and each time it happens a part of you thinks, one day this will be me. There will be people huddling round my bed deciding whether or not to resuscitate and I know one thing for sure: I don't want it just down to pot luck whether I end up brain damaged or even alive."
Staying alive: The 'miracle' machine
WHAT IS ECMO?
During cardiac arrest, blood cannot carry oxygen to the brain, causing brain cells to decay irreparably, making recovery uncertain. CPR, in which circulation is manually stimulated to delay brain damage, has long been considered the last chance for patients. With ECMO, however, those same patients can be brought back from the brink and kept alive while doctors work towards diagnosis and treatment, making CPR seem primitive by comparison. This hi-tech method of resuscitation is known as ECPR and could mark a revolution in medical practice if adopted by hospitals worldwide.
During cardiac arrest, blood cannot carry oxygen to the brain, causing brain cells to decay irreparably, making recovery uncertain. CPR, in which circulation is manually stimulated to delay brain damage, has long been considered the last chance for patients. With ECMO, however, those same patients can be brought back from the brink and kept alive while doctors work towards diagnosis and treatment, making CPR seem primitive by comparison. This hi-tech method of resuscitation is known as ECPR and could mark a revolution in medical practice if adopted by hospitals worldwide.
HOW DOES IT WORK?
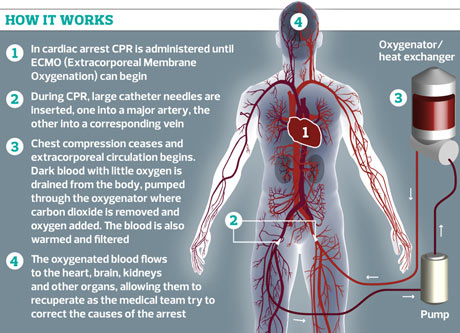
An extracorporeal membrane oxygenation machine (ECMO) is an advanced life-support apparatus. Two catheter needles are inserted, one into a major vein and one into a major artery, allowing a synthetic pump to begin drawing blood out of the body, circulating it through the apparatus, before returning it to the bloodstream. The blood passes through a membrane oxygenator, in which oxygen is introduced and carbon dioxide removed, much like the exchange of gases that takes place in the lungs. Some ECMO machines also include a heat exchanger, which can cool or warm the blood according to the patient's condition.
An extracorporeal membrane oxygenation machine (ECMO) is an advanced life-support apparatus. Two catheter needles are inserted, one into a major vein and one into a major artery, allowing a synthetic pump to begin drawing blood out of the body, circulating it through the apparatus, before returning it to the bloodstream. The blood passes through a membrane oxygenator, in which oxygen is introduced and carbon dioxide removed, much like the exchange of gases that takes place in the lungs. Some ECMO machines also include a heat exchanger, which can cool or warm the blood according to the patient's condition.
A dedicated team is required to place a patient on ECMO but, once that patient is stabilised, the machine can be supervised by specially trained nurses and can maintain stability for sustained periods. This allows the patient to live without a functioning cardiopulmonary system for days or even weeks, giving diseased organs a valuable holiday in which to recover.
WHEN IS IT USED?
Until recently, it has been used largely for severe lung failure in babies. In the UK, it is principally thought of as an intensive care treatment used in the ward, but more and more US hospitals are adding ECPR to their emergency treatment options. In an emergency, when a patient has shown no return of spontaneous circulation after conventional CPR, a doctor would decide whether the patient merits being attached to an ECMO machine, which must be carried out in a matter of minutes. Emergency ECMO is therefore administered as a last resort to patients who stand a good chance of full recovery.
Until recently, it has been used largely for severe lung failure in babies. In the UK, it is principally thought of as an intensive care treatment used in the ward, but more and more US hospitals are adding ECPR to their emergency treatment options. In an emergency, when a patient has shown no return of spontaneous circulation after conventional CPR, a doctor would decide whether the patient merits being attached to an ECMO machine, which must be carried out in a matter of minutes. Emergency ECMO is therefore administered as a last resort to patients who stand a good chance of full recovery.
In these conditions, it can be very effective and patients who have been medically dead for hours have been resuscitated successfully through ECMO, which can restart the heartbeat through steady pressure and blood flow. Even after full cardiac arrest, in situations where cell decay and brain damage have been avoided, ECMO has proved a lifesaver. There are four ECMO centres in the UK. Europe's largest centre and the only one in the UK that treats adults is the Glenfield hospital in Leicester.